3. Replacement of a damaged crown by magnetic attachment to improve dental esthetics
Tomohiro Ando, Hiroshi Mizutani
Section
of Removable Prosthodontics,
Introduction
The aim of prosthetic treatment is to restore damaged morphology and function. But cosmetic disturbance frequently results from prosthetic devices, particularly removable partial denture.
In this case report, we fabricated a removable partial denture using magnet attachment to improve dental esthetics.
Initial Situation
The patient (51-years-old, female) complained of detachment of 44, 45 cantilever bridge (Fig.1). In the past radiograph of the bridge (Fig.2), the unfavorable anatomy of 44, 45 roots, insufficient length of posts and caries of 45 tooth can be seen. Distal extension bridge and increased occlusal load from natural antagonists could be considered as reasons of bridge failure as well.
Materials and
Methods
|
|
|
|
|


Dental condition
|
|

Fig.1 Detached
extension bridge
|
|

Fig.2 X-ray photo before detaching
Treatment Planning and Procedures
The 45 tooth was indeed damaged by caries and was extracted. The restoration of 44 tooth by crown and subsequent fabrication of removable partial denture was contraindicated, because 44 tooth could not provide adequate support and was exposed to be fractured. The partial overdenture construction was indicated. At first the patient fit the lower immediate partial denture (T-bar on 43, double Akers clasps on 33, 34 were designed) (Fig.3), but the patient complained bad-looking clasps. So in order to avoid cosmetic disturbance and due to limitation of vertical space, the application of magnetic attachment was selected. The 44 root was prepared for root cap with creating ferrule effect in order to strengthen abutment (Fig.4). The root cap with cast bonded keeper Hicorex Super J 4015 was made and cemented with adhesive resin Super-Bond C&B (Fig.5). Note the limitation of vertical space available. The new lower partial overdenture was fabricated. The bracing of the denture was not enough only with this one abutment and the indirect retainer by double Akers clasps were designed on 34, 35 teeth (Fig.6). As small mechanical retention provided by the indirect retainer and root cap was enough, it was postponed to embed the magnetic assembly in the denture. After having conditioned the oral tissue for 3 months, the magnetic assembly was embedded in the denture by brush-up technique with auto polymerizing resin (Fig.7). The oral hygiene and importance of maintenance was emphasized. The patient was satisfied with denture retention comfortable mastication and sensuousness.
Fig.3 Immediate removable partial denture
|
|

Fig.4 Prepared 44 tooth for the magnetic attachment
|
|

Fig.5 A metal cap with the keeper
|
|

Fig.6 A new fabricated lower denture
|
|
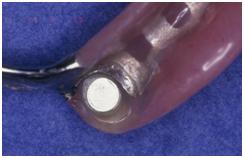
Fig.7 The magnetic assembly was embedded
Outcome of Treatment
Three years after the denture setting, displacement of lower partial overdenture was detectable and the denture was relined intraorally (Fig.8). The radiograph of 44 abutment didn’t indicate any changes in bone level or periodontal disease (Fig.9). Five years after the denture setting, the magnetic attachment had no clinically significant loss of retention, though minor scratches could be seen on surface of keeper (Fig.10). Seven years after the denture setting, the patient addressed the clinic with complaint of broken artificial tooth (Fig.11). The increased occlusal loads and insufficient thickness of acrylic resin due to space limitation were the main reason of failure. To increase resistance of 44 artificial tooth, an acrylic faced metal cast crown enable to contain the magnetic assembly were employed. Initially the impression of lower dental arch was taken with this lower denture. Then, acrylic denture base with artificial teeth were removed from the framework and cast crown was fabricated and laser welded to the framework (Fig.12). The acrylic denture base with artificial teeth and acrylic facing cast crown were processed on the framework and Hicorex Hyperslim 4013 magnetic assembly embedded by auto polymerizing acrylic resin. The partial overdenture was seated in the mouth and is in use without any problems (Fig.13). Four times a year the patient is scheduled for scaling and re-checking fit of partial overdenture. Minimal bone loss and good marginal fit could be seen in the radiograph done 10 years after root cap placement (Fig14).
|
|

Fig.8 The denture set in the mouth 3 years after first insertion3 years after the denture setting.
|
|
Fig.9 X-ray photo of 44 abutment tooth
|
|
Fig.10 Occlusal surface of the keeper 5 years after the denture setting.
|
|

Fig.11 The artificial tooth was broken.
|
|

Fig.12 A new cast crown laser welded to the lower pre-existing metal framework.
|
|

