Application of cast iron-platinum keeper to
collapsed denture for a patient with constricted oral opening: A case
report
Chikahiro OHKUBO, DMD, PhD1, Yoshihiro MAEDA, SDT2,
Ikuya WATANABE, DDS, PhD3, Naoki BABA, DDS, PhD4,
Yasuhiro TANAKA, BS, MS5, Toshio HOSOI, DDS,
PhD6
1Instructor,
Department of Removable Prosthodontics, Tsurumi University School of Dental
Medicine
2Instructor, The Dental Technician Training Institute,
Tsurumi University School of Dental Medicine
3Assistant Professor,
Department of Biomaterials Science, Baylor College of Dentistry, Texas A&M
University System Health Science Center
4Visiting Scientist,
Department of Biomaterials Science, Baylor College of Dentistry, Texas A&M
University System Health Science Center
5Instructor, Department of
Biomaterials Science, Nagasaki University Faculty of
Dentistry
6Dean, Tsurumi University School of Dental
Medicine
Chikahiro
Ohkubo
Department of Removable Prosthodontics
Tsurumi University School of
Dental Medicine
2-1-3 Tsurumi Tsurumi-ku
Yokohama 230-8501, Japan
PH:
+81-45-581-1001
Fax: +81-45-573-9599
e-mail: Okubo-c@tsurumi-u.ac.jp
Corresponding
author
Introduction
Dental practitioners must occasionally treat patients
with constricted oral openings that are caused by temporomandibular joint (TMJ)
dysfunction syndrome, rheumatoid arthritis, or damage to the masticatory muscles
by craniotomy.1 As the size of the oral opening decreases, the
difficulty of the required treatment increases. In cases when the opening is
less than 20 mm, most dental instruments cannot be inserted into the
mouth.2 Even if the patient can open his/her mouth to 30 mm, it is
very difficult to insert or remove a large conventional removable partial
denture (RPD) or complete denture (CD). There have been several
reports3-11 regarding prosthodontic treatment for medically
compromised patients, including patients with limited intraoral access
(microstomia, resected cancer patients, etc.). Sectional dentures and/or
collapsed dentures have usually been prescribed for these
patients.3,5,8,11 A hinge is used to connect the segments of such a
collapsed denture system.3,11 Other methods of assembling the two
segments of sectional dentures are clasps,3-5 cast locking
recesses,5 swing-lock attachments,11 pin
attachments,8 and a telescope system.11
Recently an
attachment system using magnets has been developed, and several types are
commercially available for retention of overdentures or implant-retained
prostheses.12-14 Also it has been found that Fe-Pt alloys have
magnetic properties, and the possibility of applying them to dentistry has been
investigated. Watanabe et al.13 reported that cast Fe-Pt keeps yield
great attractive force to dental Fe14Nd2B magnets (Fig.
1). Additionally, Fe-Pt alloys exhibit excellent corrosion resistance because
they contain a large amount of platinum (approximately 70 wt% Pt).14
The great advantage of this system is that they can be cast using a dental
casting machine and any size or shape of keeper can be fabricated. Thin (less
than 1 mm) or specially shaped keepers are needed in each particular
case.
This clinical report describes the application of a Fe-Pt keeper to a
collapsed RPD for a patient with an extremely constricted oral opening.
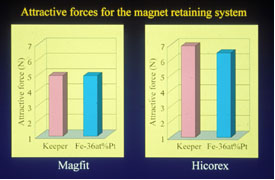
Fig. 1 Attractive force to dental Fe14Nd2B
magnets
CLINICAL REPORT
The patient was a 69-year-old partially edentulous woman
with missing posterior teeth, namely, two right molars and two premolars, two
left molars, and the first premolar, of the mandibular (eight teeth, #17, #21 to
#27 remained in the mandibular arch) (Figs. 2a-c). Her oral opening had been
gradually constricted by rheumatoid arthritis for approximately 20 years. The
oral opening became even more constricted after amputation of her temporal
muscle by craniotomy for a subarachnoid hemorrhage in October 1999. The size of
the oral opening was less than 15 mm at her first visit to the division of
Maxillo-facial Oral Surgery of our dental school hospital in December 1999. In
this division, the patient was trained for one year at opening her mouth using
an oral expansion device (Figs. 3a, 3b). When she visited the division of
Prosthodontics, she was able to open her mouth approximately 25 mm. She had an
extremely small RPD that was unserviceable when the denture flanges and clasps
were removed.
Figs. 2 a-c Intraoral view of a partially edentulous
patient
Figs. 3 a, b Severely constricted oral opening due to rheumatoid
arthritis and craniotomy.
Impression and wax denture fabrication
Preliminary impressions for both
dental arches were made using a sectional stock tray (Figs. 4a-d). This tray was
developed from a full arch tray sectioned into right and left halves and could
be reconnected using a slide-lock system on the tray handle.17 A
border molding and definitive impression was also made using a sectional custom
tray with slide-lock joint (Figs. 5 a-c).2 The upper and lower jaw
relationship was registered using a sectional occlusion rim with a dowel-pinhole
joint (Fig. 6). The master casts were mounted on an average valued articulator
(Gysi Simplex OU-II, Onuki-Iki, Tokyo, Japan), and the artificial teeth
(Duradent, GC Corp., Japan) were conventionally arranged. The wax denture could
be collapsed on the right denture base with a clip hinge (Binder clip 36,
Kokuyo, Osaka, Japan) as shown in Fig. 7. The feasibility of placement and
removal of the final prosthesis was carefully confirmed using this wax
denture.
Figs. 4 a-d Preliminary impressions were made using a sectional stock
tray
Figs. 5 a-c Definitive impressions was made using a sectional custom
tray
Fig. 6 Jaw relationship was registered using sectional occlusion rim
with a dowel-pinhole joint
Fig. 7 Wax denture collapsed in the right denture base with clip
hinge.
Denture designs
The right distal extension base of the denture was
composed of upper and lower segments, which were collapsed using a hinge
(Swing-lock attachment, Idea Development Co., Dallas, TX) at the edge of the
lingual flange, allowing for insertion into the mouth (Fig. 8). The metal
frameworks of both segments were separately cast with Co-Cr-Ti alloy (Crutanium,
Krup Inc., Essen, Germany). The clearance was too small (approximately 4 mm in
the thinnest region) between the maxillary natural teeth and mandibular residual
ridge to place commercial attachments connecting the two segments. Also the
shape of the keeper fitted to the framework and residual ridge was complicated.
Therefore, a cast Fe-Pt keeper (Fe-66.3 wt% Pt) and the thinnest commercial
magnets available (Hicorex-slim, Hitachi Metals, Japan) were used for this
case.
Fig. 8 Schematic drawing of the right distal base composed of upper and
lower segments, collapsed using hinge.
Denture fabrication
The wax pattern for the lower segment including a
plastic pattern of the convex hinge was designed to be assembled with the keeper
and was fabricated on the refractory cast. The pattern was invested (Crutavest,
Krup Inc.,) and cast with Co-Cr-Ti alloy in a centrifugal casting machine (Grove
Cast, Krup, Inc.). After it was desprued and polished, the lower framework was
replaced on the master cast, and the Fe-Pt keeper pattern was then made. The
keeper pattern was invested in a mold with a magnesia-based investment (Selevest
CB, Selec Co., Osaka, Japan) and cast from a custom-made Fe-Pt ingot using a
high-frequency centrifugal casting machine (Jelenko Eagle, Jelenko, NY). After
casting, the Fe-Pt keeper underwent heat treatments in accordance with
procedures reported by Watanabe et al.13,14 The cast Fe-Pt keeper was
then welded to the Co-Cr-Ti lower framework using a laser (neolaser L ALC 30,
Selec Co.). The pattern for the upper segments of the framework with a concave
hinge was fabricated and cast with the same alloy in the same manner as for the
lower framework. After the upper framework was polished, the concavo-convex
hinge was laser-welded to join the two frameworks (Figs. 9 a-f). Denture-base
PMMA resin (Palapress Vario, Heraeus Kulzer Inc, Irvine, Calif.) was polymerized
for the upper and lower segments according to the manufacturer's instructions.
Three commercial magnets (Hicorex-slim) were embedded under the metal teeth in
the upper segment with auto-polymerized resin (Uni-fast 2, GC Corp. ). Figure 10
show the final RPD, which could be collapsed using a lingual flange hinge and
magnetic attachments.
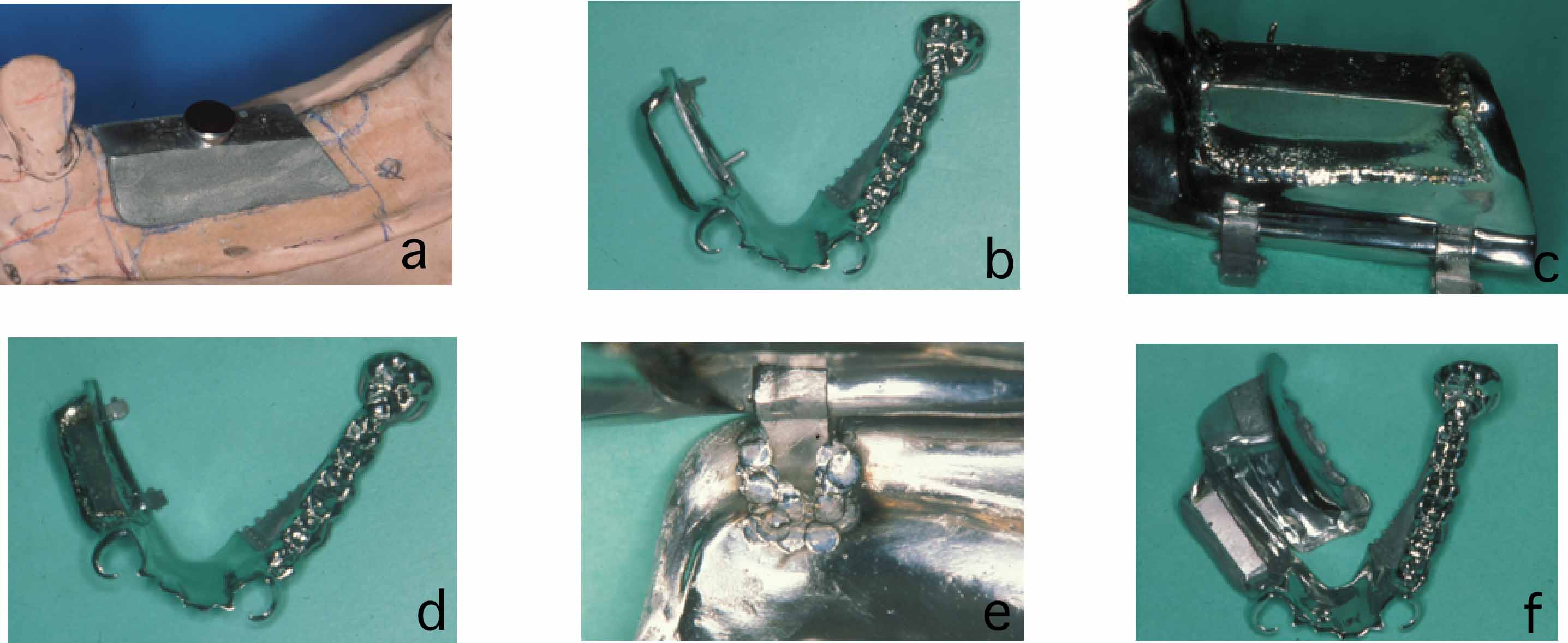
Figs. 9 a-f Assembled framework of upper and lower segments by laser
welding
Figs. 10 a, b Completed RPD could be collapsed using lingual flange
hinge and magnetic attachments.
Delivery of dentures
The denture was inserted in the mouth by collapsing
the right denture base to the lingual side. After being inserted into the mouth,
the upper segment was rotated and connected to the lower segment. The denture
was fitted after it was restored to its original form in the mouth (Figs. 11a,
11b). Figure 12 shows an occlusal view of the denture after placement.
After
an observation period of 1 year and 2 months, the collapsed denture, which was
easily inserted into the mouth, continues to deliver adequate function with no
problem, and the patient is very satisfied.
Figs. 11 a, b Delivery of collapsed denture into the
mouth.
Fig.12 Occlusal view of the lower arch after installation of collapsed
denture.
SUMMARY
This report described a removable collapsed denture connected by
hinges and a magnetic retention system consisting of a cast iron-platinum keeper
and commercial magnet (Hicorex-slim) for a patient with a severely constricted
oral opening. With the use of a cast keeper and flange hinges, the collapsible
RPD was successfully and easily installed, and the patient expressed
satisfaction regarding her masticatory function.
ACKNOWLEDGMENTS
Editorial assistance by Mrs. Jeanne Santa Cruz is
greatly appreciated.
REFERENCES
1) Fricton JR, Kroening RJ, Hathaway KM. TMJ and craniofacial
pain: Diagnosis and management. Ishiyaku EuroAmerica, Inc. S. Louis, 1-11,
1988.
2) Ohkubo C, Maeda Y, Sugiyama K, Suzuki Y, Ishikawa Y, Hosoi T.
Impression techniques for patients with microstomia or constricted oral opening.
Tsurumi Univ Dent J 28: 145-151, 2002.
3) Conroy B, Reitzik M. Prosthetic
restoration in microstomia. J. Prosthet. Dent. 26: 324。チ327, 1971.
4) Hagiwara
H, Nakamura H, Matsumura M, Seto K, Abe K, Nomura T. The mouth circumference of
normal adults and patients of microstomia. J Jpn Maxillofacial Prosthet 5:
37-43, 1982.
5) Winkler S, Wongthai P, Wazney JT. An improved split-denture
technique. J. Prosthet. Dent. 51: 276-279, 1984.
6) Luebke RJ. Sectional
impression tray for patients with constricted oral opening. J. Prosthet. Dent.
52: 135。チ137, 1984.
7) Whitsitt JA, Battle LW. Technique for making flexible
impression trays for the microstomic patient. J. Prosthet. Dent. 52: 608。チ609,
1984.
8) McCord JF, Moody GH, Blinkhorn AS. An overview of dental treatment
of patients with microstomia. Quintessence Int. 21: 903。チ906, 1990.
9)
Mirfazaelian A. Use of orthodontic expansion screw in fabricating section custom
trays. J. Prosthet. Dent. 83: 474。チ475, 2000.
10) Baker SP, Brandt RL,
Boyajian G. Impression procedure for patients with severely limited mouth
opening. J. Prosthet. Dent. 84:241。チ244, 2000.
11) Suzuki Y, Abe M, Hosoi T et
al. Sectional collapsed denture for a partially edentulous patient with
microstomia: A clinical report. J Prosthet. Dent. 84: 256。チ259, 2000.
12)
Kurtz KS, Ohkubo C, Watanabe I Shimizu H, Cai Z, Okabe T. Evaluation of magnet
system retaining a midfacial maxillofacial prosthesis. J Dent Res 79: 178(Abstr.
277), 2000.
13) Watanabe I, Tanaka Y, Fukunaga H, Hisatsune K, Atsuta M.
Attractive force of castable iron-platinum magnetic alloys. Dent Mater
17:197-200, 2001.
14) Watanabe I, Hai K, Tanaka Y, Hisatsune K, Atsuta M. In
vitro corrosion behabior of cast iron-platinum magnetic alloys. Dent Mater
17:54-61, 2001.
15) Mastumoto Y, Abe M, Hosoi T, Mizuno Y. Removable
prosthesis using hinge in distal-end for path of insertion. J. Jpn. Soc. Magnet.
Applicat. Dent. 9:17-22, 2000.
16) Mastumura H, Kawasaki K. Magnetically
connected removable sectional denture for a maxillary defect with severe
undercut: A clinical report. J. Prosthet. Dent. 84:22-6, 2000.
17) Ohkubo C,
Ohkubo C, Hosoi T. Development of sectional stock tray system. The Nippon Dental
Review. 61: 103-105, 2001.