INTRODUCTION
Microstomia
is often a sequela of burns, postoperative
head and neck trauma, surgical
resection of facial and oral neoplasms, and
scleoderma.1 The
patients who must wear removable dental prostheses
often complain of an
inability to insert or remove a denture due
to constricted opening. There have
been several reports regarding the fabrication
of removable prostheses for
patients with mictostomia. Some include the
use of Co-Cr frameworks with clasps
to hold sectional complete dentures,2,3 a sectional complete denture
joined by a post that slides into stainless
steel tubing,4 and use
of cast Co-Cr hinges and swing-lock attachments
for removable partial or
complete dentures.5,6 There are few reports about sectional complete
dentures utilizing dental magnetic attachments.
Matsumura and Kawasaki7
utilized a dental magnetic attachment for
a sectional removable partial denture
for a patient with a severe undercut secondary
to ablative tumor surgery. They
reported that the magnetic retention system
is considered to be clinically
useful for interrelating and retaining a
segmented sectional prosthesis.
Currently, there are several commercially
available magnetic attachment systems
for use in clinical dentistry. Recently,
it has been found that Fe-Pt alloys
have magnetic properties,8-10 and they have been investigated for possible
application to
dentistry.11,12 Watanabe et al.13,14 developed the Fe-Pt magnetic
attachment system. They reported that the
cast Fe-Pt keeper yielded great
attractive force to dental Fe14Nd2B magnet.13 Furthermore, the Fe-Pt alloys
exhibit excellent corrosion resistance because
they contain a large amount of
platinum (approximately 70wt% Pt).14 Since the Fe-Pt alloys can be
cast in a dental casting machine, any size
or shape of castable magnetic
attachment can be fabricated for prostheses.
The cost of platinum for custom
magnetic castings is comparable to the cost
of commercially available magnetic
prosthetic components. Clinical indications
include magnetic retention for
conventional intraoral dental prostheses
and intra or extraoral maxillofacial
prostheses. Implant retained maxillofacial
prostheses often have anatomically
confounding factors which require custom
castings to align prosthetic retentive
components and allow a favorable path to
insertion. Kurtz et al.12
have investigated and demonstrated efficiency
of this concept. The custom cast
Fe-Pt magnetic attachment , therefore, has
a variety of custom applications as
compared to the commercially available dental
magnetic attachment.
This
clinical report describes the prosthodontic
treatment of an edentulous patient
with microstomia induced by scleroderma using
cast Fe-Pt magnetic attachments.
CLINICAL REPORT
A
67-year-old edentulous woman with microstomia
induced by scleroderma presented
for prosthetic evaluation (Fig. 1). The diameter and circumference of
her mouth were approximately 32 mm and 95
mm, respectively. The patient had
extremely small complete dentures which were
unserviceable and refused to
undergo surgical enlargement of the mouth
aperture.

Fig. 1. Diameter and circumference of
patient=s mouth was approximately 32 mm and 95 mm,
respectively, because of
scleroderma.
Impression and wax denture
fabrication
Preliminary
impressions with two stock impression trays
of each half of the mouth for both
dental arches, fabrication of sectional custom
trays for the final impressions,
border molding and final impressions were
accomplished according to the
previous reports.6 The jaw relationship was recorded with sectional
collapsed occlusion rims fabricated with
autopolymerizing PMMA base resin (Tray
resin, Shofu Inc., Kyoto, Japan), commercial
dental magnetic attachments
(Hicorex 4513, Morita Corp., Kyoto, Japan)
and clip hinges (Binder clip 36,
Kokuyo, Osaka, Japan). The master casts were
mounted on an average valued
articulator (Dental Hobby, Shioda Co. Ltd.,
Tochigi, Japan), and artificial
teeth (Endura, Shofu Inc., Kyoto, Japan)
were conventionally arranged. The wax
dentures could be sectioned and collapsed
as shown in Fig. 2. The
anterior segments included artificial teeth
of incisors and both canines, and
could be connected to the posterior segments
using dental magnetic attachments.
The posterior segments could be collapsed
using hinges located at the center of
the denture bases. Using the upper and lower
sectional collapsed wax dentures,
the correct jaw relationship was confirmed
in the patient=s mouth. Placement and removal of
the trial prosthesis was rehearsed and with
practice and could be easily
accomplished by the patient.

Fig. 2. Sectional collapsed trial dentures fabricated
with clip hinges and dental magnetic attachments.
Denture designs
Each denture was composed of an
anterior and two posterior segments. Anterior
segments include artificial teeth
of incisors and both canines, and cast Fe-Pt
magnet (Fe-69.3%Pt-0.6%Nb).
Posterior segments include bilateral premolars
and molars, and cast Fe-Pt
keeper (Fe-66.3%Pt). Cast Co-Cr (Partial
Denture Alloy, Jelenko, NY) (Co:63.0%,
Cr: 28.5%, Mo:6.0%) metal frameworks were
built into all of the segments except
for an anterior segment of the lower denture.
The Co-Cr metal frameworks of
posterior segments could be collapsed using
the lingual and palatal midline
hinges (Swing-lock attachment, Idea Development
Co., Dallas, TX) which allowed
for insertion into the mouth (Fig. 3). The anterior segments could be
connected to/from the posterior segments
due to the Fe-Pt magnets and keepers.

Fig. 3. Co-Cr metal frameworks that can
collapse using lingual and palatal midline hinges.

Fig. 4. Cast Fe-Pt magnet with concavo design.
Denture fabrication
The
left half wax pattern of the Co-Cr framework was fabricated on a
phosphate-bonded refractory cast (Snow White, Shofu Inc., Kyoto Japan) and the
plastic pattern of the concave hinge cylinder was placed and embedded at the
lingual or palatal midline of the framework wax pattern. The half pattern of
framework and hinge were cast with the Co-Cr alloy using a vacuum induction
casting machine (Argon Caster, Shofu Inc., Kyoto, Japan). After polishing the
cast framework of the left half, the framework was returned on the master cast.
Right half wax pattern of framework and wax pattern of convex hinge were then
fabricated on the refractory cast in which left half framework was embedded,
and cast with the Co-Cr alloy. These procedures followed manufacturer=s instruction for fabrication of the
swing-lock attachment hinge. The patterns of the Fe-Pt keeper were fabricated
on the master cast on which the polished Co-Cr framework has been returned. A
pattern of the Co-Cr framework for anterior segment of upper denture was also
made on the polished Co-Cr framework seated on the master cast and was cast
separately. The patterns of Fe-Pt keeper were invested in a mold with a
magnesia-based investment (Selevest C&B, Selec Co., Osaka, Japan) and cast
with custom-made Fe-Pt ingot using a centrifugal high-frequency casting machine
(Jelenko Eagle, Jelenko, NY). The wax patterns for cast Fe-Pt magnetic
attachment were designed convex for the keeper and concave for the magnet
components (Figs. 3 and 4). This concavo-convex design allows for rigid
connection of the anterior segment to the posterior segment. The patterns of
Fe-Pt magnet were made on the polished cast Fe-Pt keeper on the master cast and
fabricated in the same manner as the Fe-Pt keeper. Figure 4 demonstrates
the Fe-Pt magnets after casting. The Fe-Pt keepers and magnets underwent heat
treatments according to the previous study reported by Watanabe et al13
,14 and Kanno et al.15 The Fe-Pt
magnets were magnetized using a magnetizer
(MSD-200-3500P, Nihonkokan, Tokyo,
Japan) after heat treatment. The cast Fe-Pt
keepers were then laser-welded
(TLL7000, Tanaka Laser Co., Tokyo, Japan)
to the Co-Cr framework as shown in Fig.
3. After the preparation of Co-Cr frameworks
and Fe-Pt magnetic
attachments, denture-base PMMA resin (New
Modern Core, Sankin, Tokyo, Japan)
for the anterior segment and posterior segment
were polymerized separately in
accordance with the manufacturers directions.
The cast Fe-Pt magnets were
embedded in the anterior segments when the
base-resin was polymerized. Figure
5 shows the final complete denture prostheses.
The dentures could be
sectioned and collapsed due to the lingual
and palatal midline hinges and the
Fe-Pt magnetic attachments.
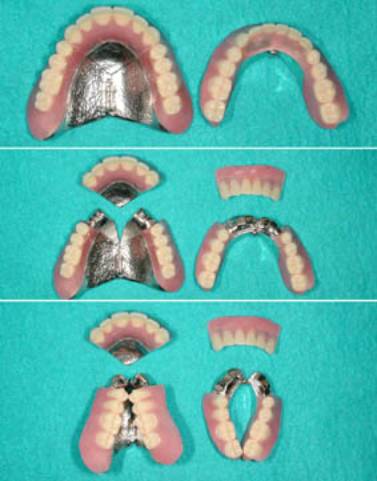
Fig. 5. Final sectional collapsed
complete dentures.
Delivery of dentures
The
patient was given home care instruction on
the operation of the sectional
collapsed complete dentures. Since it is
impossible for the patient to deliver
the dentures into the mouth without sectioning
and collapsing, collapsed
posterior segments are first delivered into
the mouth (Fig.6). Then, the
sectioned anterior segments are delivered
and connected to the posterior
segments in the mouth as shown in Fig. 7. Figure 8 shows a
frontal view of the patient after installation
of upper and lower sectional
collapsed complete dentures.

Fig. 6.
Delivery of the collapsed posterior segments.

Fig. 7.
Delivery of the sectioned anterior segments.

Fig. 8. Frontal view of the patient after installation
of upper and lower dentures.
DISCUSSION
Fe-Pt
dental magnetic attachments are clinically
useful for retention of prostheses
due to excellent attractive force. Since
the attachment keeper is placed onto
the root canal of the abutment tooth or implant
abutment, the size of the
keeper and its magnet are circumscribed by
the size of the abutment tooth or
implant abutment. Therefore, several sizes
of magnets and keepers are available
in prefabricated commercial dental magnetic
attachment systems. However,
prefabricated magnetic components are designed
(flat-on-flat). This allows for
easier displacement by a force parallel to
the flat connection plane. Since the
Fe-Pt magnetic attachment system (magnet
and keeper) can be cast in a dental
casting machine, any size or shape of castable
magnetic attachment can be
fabricated for prostheses. Because of the
castable property of Fe-Pt magnetic
attachment, the wax patterns for cast Fe-Pt
magnetic attachment were designed
convex for the keeper and concave for the
magnet (Figs. 3 and 4). This
concavo-convex design rigidly connect the
anterior segment to posterior segment
and prevents wear of the magnetized components and stress concentration
at the lingual and palatal midline hinge
during chewing functions. This
prevents denture deflection and may minimize
the possibility of breakage.
The
Fe-Pt magnetic attachment (magnet and keeper)
requires heat treatments to
obtain magnetic properties after casting.
The magnetic properties can be
achieved due to the
order‑disorder phase transformation
of the binary Fe‑Pt alloy system.11
The Fe-Pt keeper requires solution heat treatment
to produce the disordered
Fe-Pt atoms. The ordered Fe-Pt magnet can
be acquired by aging heat treatment
after solution treatment. Then, the Fe-Pt
magnet has to be magnetized to
arrange the direction of ordered Fe-Pt atoms.
After obtaining magnetic
properties, other heat effects such as soldering
and brazing reduce the
magnetic properties, resulting in the decrease
of the attractive force between
the Fe-Pt magnet and keeper. Therefore, laser-welding
applied in this case (Fig.
3) is the most favorable method to weld the
Fe-Pt magnet or keeper to the
other alloys. Since laser energy can be concentrated
on a small area, there are
fewer effects of heating and oxidation on
the area surrounding the spot to be
welded.16 If
the Fe-Pt magnets lose magnetic properties
after clinical use due to the
circumferential magnetic field, they can
be remagnetized to restore the
attractive force without any damage to the
denture components.
The
magnetically connected sectional prostheses
described in this clinical report
is convenient for this patient in terms of
insertion/withdrawal, and has
functioned very favorably for a service period
of one year. No visible fracture
or wear has been observed in this magnetic,
hinged, collapsable prostheses.
Follow-up appointments to monitor prostheses
function or treatment
complications will continue.
SUMMARY
This
clinical report described cast iron-platinum
magnetic attachment system applied
to sectional collapsed complete dentures
for an edentulous patient with
microstomia. With the use of the lingual
and palatal midline hinges and Fe-Pt
magnetic attachment, the sectional collapsed
complete dentures could be
successfully and easily installed and delivers
adequate function in the patient=s mouth.
REFERENCES
1. Smith PG, Munts HR, Thawley SE. Local
myocutaneous advancement flaps. Alternative
to cross-lip and distant flaps in the recocstruction
of ablative lip defects. Arch Otolaryngol
1982;108:714-8.
2. Conroy B, Reitzik M. Prosthetic restoration
in microstomia. J Prosthet Dent 1971;26:324-7.
3. Winkler S, Wongthai P, Wazney JT. An improved
split denture technique. J Prosthet Dent
1984;51:276-9.
4. MacCord JF, Tyson KW, Blair IS. A sectional
complete denture for a patient with microstomia.
J Prosthet Dent 1989;61:645-7.
5. Wahle JJ, Gardner LK, Fiebiger M. The
mandibular swing?lock complete denture for
patients with microstomia. J Prosthet Dent
1992;68:523-7.
6. Suzuki Y, Abe M, Hosoi T, Kurtz K. Sectional
collapsed denture for a partially edentulous
patient with microstomia: A clinical report.
J Prosthet Dent 2000;84:256-9.
7. Matsumura H, Kawasaki K. Magnetically
connected removable sectional denture for
a maxillary defect with severe undercut:
A clinical report. J Prosthet Dent 2000;84:22-6.
8. Watanabe K, Masumoto H. On the high energy
product of Fe?Pt permanent magnet alloys.
J Jpn Inst Metals 1983;47:699-703.
9. Watanabe K. Permanent magnet properties
in Fe-Pt-Nb system alloys. J Jpn Inst Metals
1990;54:1284-90.
10. Watanabe K. Permanent magnet properties
and their temperature dependence in the Fe-Pt-Nb
alloy system. Mater Trans JIM 1991;32:292-8.
11. Tanaka Y, Kimura N, Hono K, Yasuda T.
Microstructure and magnetic properties of
Fe?Pt permanent magnets. J Mag Mater 1997;170:289-97.
12. Kurtz K, Ohkubo C, Watanabe I, Shimizu
H, Cai Z, Okabe T. Evaluation of magnet system
retaining a midfacial maxillofacial prosthesis.
J Dent Res 2000;79:178 (Abstr 277).
13. Watanabe I, Tanaka Y, Fukunaga H, Hisatsune
K, Atsuta M. Attractive force of castable
iron-platinum magnetic alloys. Dent Mater
2001;17:197-200.
14. Watanabe I, Hai K, Tanaka Y, Hisatsune
K, Atsuta M. In vitro corrosion behavior
of cast iron-platinum magnetic alloys. Dent
Mater 2001;17:217?20.
15. Kanno T, Nakayama T, Kimura K, Okuno
O. Effect of Si and Nb on Fe-Pt magnetic
casting alloys. J Jpn Soc Dent Mater Dev
1998;17:54?61.
16. Roggensack M, Walter MH, Boning KW. Studies
on laser- and plasma- welded titanium. Dent
Mater 1993;9:104-7.